Overcoupling and Undercoupling: Understanding Trauma Through a Somatic Lens
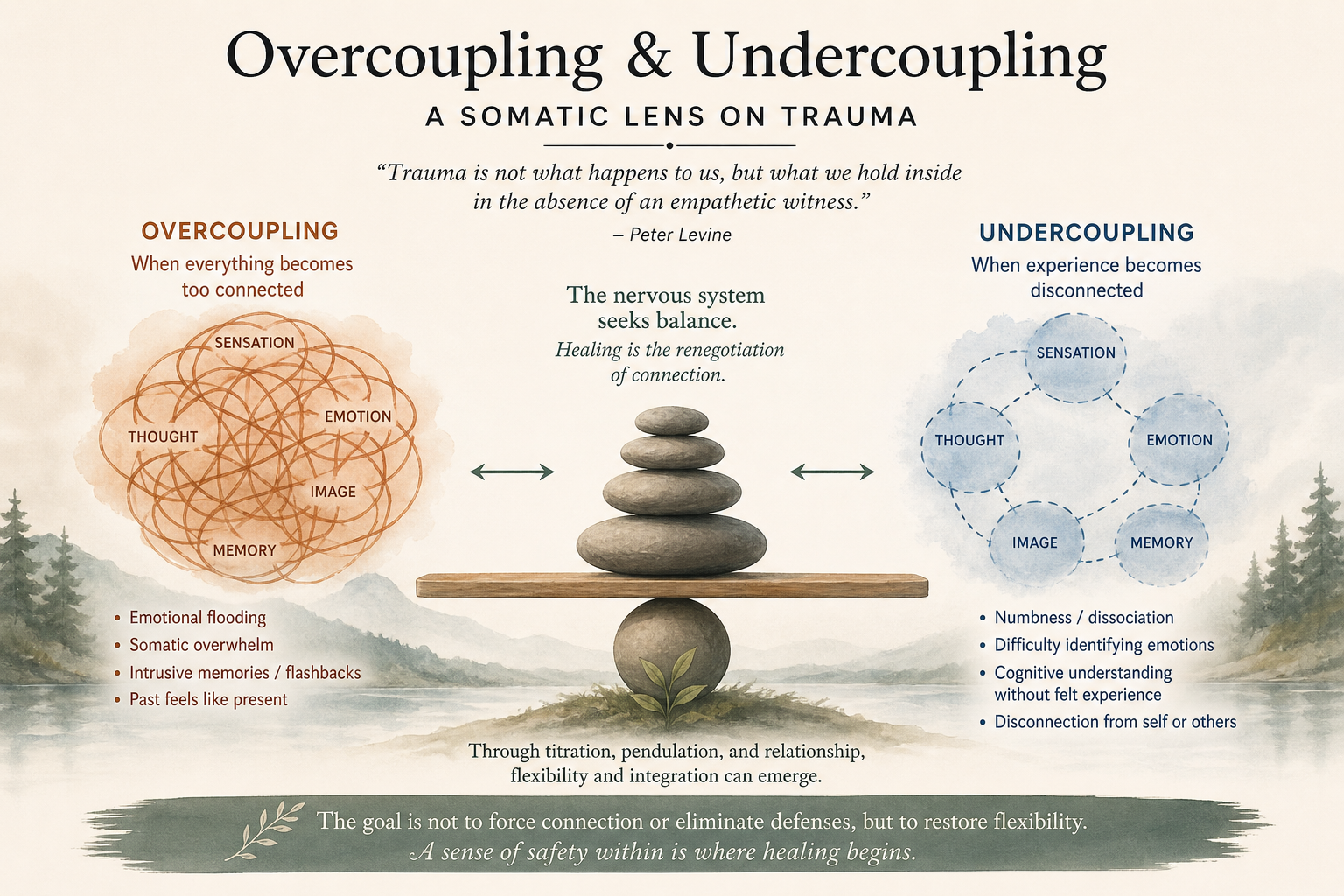
Overcoupling and undercoupling, concepts from Peter Levine, describe how trauma disrupts the nervous system’s ability to integrate experience. Overcoupling links sensations, emotions, and memories too tightly, leading to overwhelm, while undercoupling separates them, resulting in disconnection or numbness. Healing involves gently restoring flexible connections so the body can process experience without becoming flooded or shut down.
In the evolving field of trauma therapy, few voices have been as influential as Peter Levine, the developer of Somatic Experiencing®. Levine’s work invites us to look beyond thoughts and behaviors and into the body’s lived experience of trauma. Among his many contributions, the concepts of overcoupling and undercoupling offer powerful insight into how traumatic experiences become encoded—and how healing can unfold.
What Is Coupling?
At its core, coupling refers to how different elements of an experience become linked together in the nervous system (if this happens, this will follow). In a well-regulated system, experiences are integrated in a flexible and adaptive way. But trauma disrupts this process.
As Levine writes, “Trauma is not what happens to us, but what we hold inside in the absence of an empathetic witness.” When overwhelming experiences are not metabolized, the nervous system organizes itself around survival rather than integration.
This is where overcoupling and undercoupling emerge.
Overcoupling: When Everything Becomes Too Connected
Overcoupling occurs when multiple elements of a traumatic experience become fused together too tightly. A sensation, image, emotion, or thought becomes inseparable from the entire traumatic memory.
For example, a raised voice may not simply be heard as sound—it may instantly evoke fear, shame, body tension, and implicit memories of past harm. The nervous system reacts as if the past is happening now.
Levine describes this as a kind of “excessive linkage,” where “the whole is triggered by a part.”
Clinically, overcoupling often shows up as:
Emotional flooding
Somatic overwhelm (e.g., tight chest, racing heart)
Intrusive memories or flashbacks
Difficulty distinguishing past from present
In this state, clients may feel hijacked by their experience, with little access to regulation or perspective.
Undercoupling: When Experience Becomes Fragmented
If overcoupling is too much connection, undercoupling is too little.
Undercoupling occurs when aspects of experience are disconnected from one another. Emotions may be cut off from bodily sensations, or memories may feel distant, vague, or inaccessible. Some clients report vision feeling fuzzier or more vague sensation.
Levine notes that trauma can lead to “a failure to link the various elements of experience into a cohesive whole.”
This often presents as:
Numbness or dissociation
Difficulty identifying emotions
Cognitive understanding without felt experience
A sense of disconnection from self or others
In undercoupling, the nervous system protects by separating rather than overwhelming. While this may reduce distress in the short term, it can also limit the ability to process and integrate experiences over time. If we keep out emotion, we also keep out positive feelings such as joy, connection, closeness…
The Dance Between Over and Under
Importantly, these are not fixed states. Many clients oscillate between overcoupling and undercoupling—flooding one moment, numb the next. This fluctuation reflects the nervous system’s attempt to find safety.
Healing, in Levine’s framework, involves gently renegotiating these patterns.
He emphasizes titration and pendulation—working with small, manageable pieces of experience and allowing the nervous system to move between activation and settling.
As he writes, “Trauma can be resolved through the renegotiation of the nervous system.”
Clinical Implications
Understanding overcoupling and undercoupling can deepen clinical attunement and guide interventions:
With overcoupling, the goal is to uncouple—to help clients differentiate elements of their experience, orient to the present, and build capacity for regulation.
With undercoupling, the work involves gentle linking—supporting clients in reconnecting sensations, emotions, and meaning in a tolerable way.
Both require pacing, consent, and a strong therapeutic alliance.
A Somatic Path Toward Integration
Levine’s work reminds us that trauma is not simply stored in memory—it is held in the body. Overcoupling and undercoupling are not signs of pathology, but adaptations of a nervous system doing its best to survive.
When approached with curiosity and care, these patterns become entry points for healing.
Integration is not about forcing connection or eliminating defenses—it is about restoring flexibility.
And in that flexibility, clients can begin to experience something many have long been without: a sense of safety within themselves. This is the work of finding a path forward.
Attachment-Focused EMDR: Healing Through Connection and Repair
Attachment-Focused Somatic-Informed EMDR expands traditional EMDR by addressing not just trauma symptoms, but the relational wounds underlying them—especially those formed in early attachment experiences.
Grounded in attachment theory and articulated by Laurel Parnell, this approach emphasizes that trauma often occurs in relationships and must be healed within a safe, attuned relational context. It integrates somatic awareness to address pre-verbal trauma stored in the body, which may not be accessible through talk therapy alone.
While maintaining EMDR’s eight-phase structure, this model shifts the focus in several key ways: resourcing becomes relational and experiential (not just cognitive), pacing is slower and guided by the client’s nervous system, and therapeutic interventions aim to repair unmet developmental needs. The therapist’s presence—through attunement, consistency, and co-regulation—becomes a central mechanism of healing.
This approach is particularly effective for clients with complex trauma, including early neglect or abuse, chronic shame, dissociation, and relational difficulties, especially when standard EMDR has not been fully effective.
Ultimately, Attachment-Focused Somatic-Informed EMDR reframes healing as not only the reprocessing of traumatic memories, but also the experience of being safely connected, seen, and cared for—making deeper and more sustainable transformation possible.
Eye Movement Desensitization and Reprocessing (EMDR) is widely recognized as an effective, evidence-based approach for resolving trauma. Yet, as clinicians deepen their understanding of trauma, many are finding that symptom reduction alone is not always sufficient—particularly for clients with early relational wounds. This is where Attachment-Focused EMDR, developed as articulated by Laurel Parnell, in addition to Somatic Experience integration offer a meaningful expansion.
Attachment-Focused EMDR integrates the standard EMDR protocol with a relational, attuned approach that prioritizes safety, connection, and repair. It acknowledges that trauma often occurs within relationships—and therefore must also be healed within a relational context. Somatic Experience supports the reality that attachment related trauma can often occur pre-verbally, which limits the ability to verbally process trauma that is stored in implicit memory.
The Foundation: Attachment Matters
Attachment theory teaches us that early relationships shape our internal working models—how we see ourselves, others, and the world. When those early relationships are marked by inconsistency, neglect, or harm, individuals may internalize beliefs such as “I am not safe,” “I am not worthy,” or “I am alone.”
Traditional EMDR can effectively target distressing memories tied to these beliefs. However, Attachment-Focused EMDR recognizes that for many clients, especially those with complex trauma, the therapeutic relationship itself becomes a central mechanism of healing.
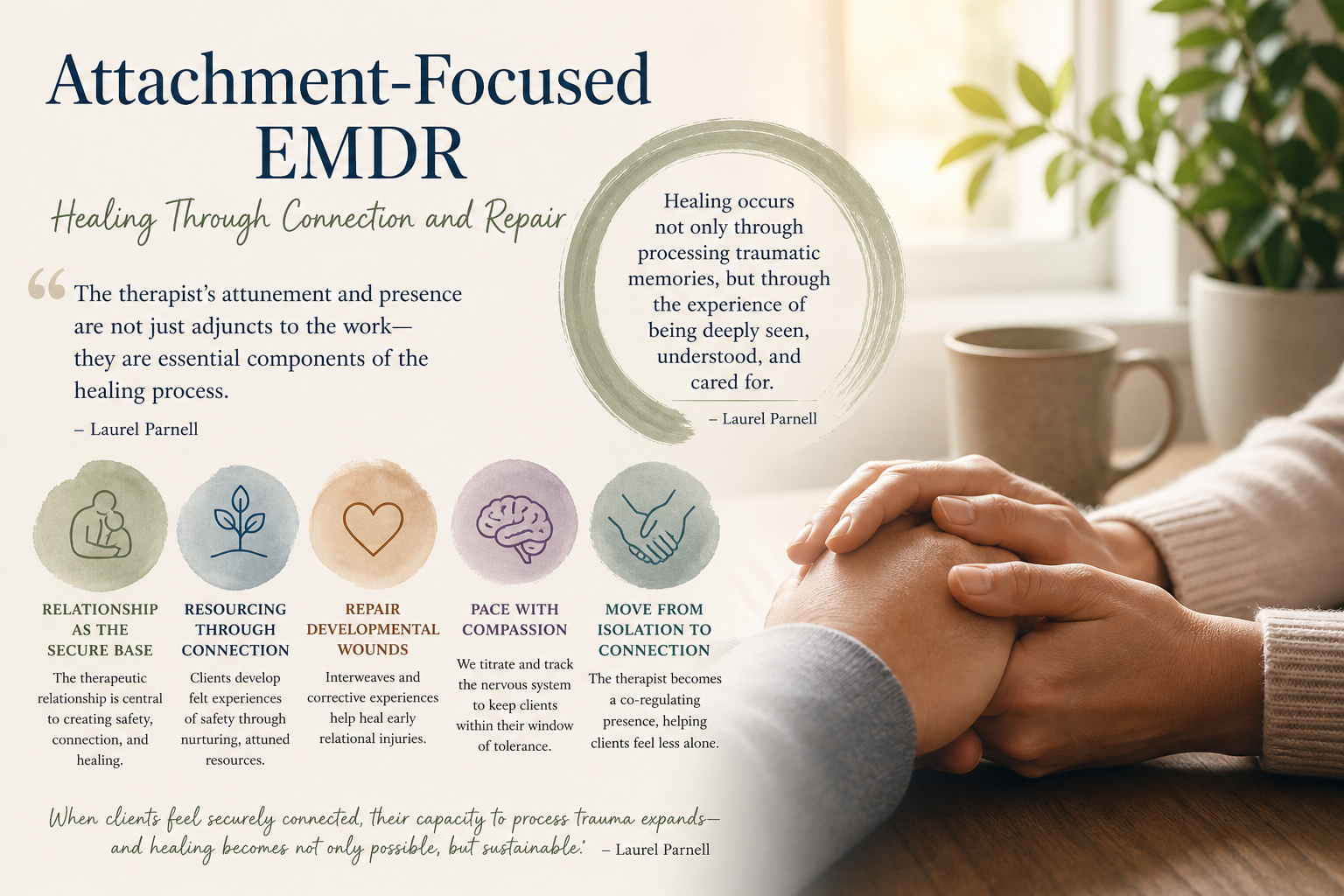
As Parnell writes, “The therapist’s attunement and presence are not just adjuncts to the work—they are essential components of the healing process.”
What Makes EMDR “Attachment-Focused”?
While maintaining the eight-phase EMDR structure, Attachment-Focused EMDR emphasizes:
Resourcing as relational, not just internal
Clients are supported in developing felt experiences of safety, often through imaginal nurturing figures, spiritual resources, or the therapist’s attuned presence.Pacing and titration
Rather than pushing for rapid desensitization, clinicians track the client’s nervous system closely, ensuring work remains within a tolerable window. Particularly with the somatic integration, there is gentle space to let the body take the lead.Repair of developmental deficits
Early unmet needs are addressed through interweaves (supportive reframes or questions that offer corrective emotional experiences.)The therapeutic relationship as a secure base
The clinician’s consistency, empathy, and responsiveness become part of the reprocessing experience itself.
Parnell emphasizes this shift, noting: “Healing occurs not only through processing traumatic memories, but through the experience of being deeply seen, understood, and cared for.”
Clinical Implications
Attachment-Focused Somatic-Informed EMDR is particularly well-suited for clients who:
Have histories of early neglect, abuse, or inconsistent caregiving
Struggle with affect regulation or dissociation
Experience chronic shame or relational difficulties
Have not responded fully to more structured or exposure-based approaches
In these cases, standard EMDR protocols may need adaptation. Attachment-Focused Somatic-Informed EMDR invites clinicians to slow down, prioritize connection, and integrate somatic and relational cues into every phase of treatment.
The Role of the Therapist
This approach asks more of the therapist—not in technique, but in presence. It requires:
Deep attunement to subtle shifts in affect and physiology
Comfort with relational closeness and repair
Willingness to integrate parts work, somatic awareness, and interweaves fluidly
Parnell highlights this beautifully: “The therapist becomes a co-regulating presence, helping the client move from isolation into connection.”
Integrating Attachment and EMDR
Attachment-Focused Somatic-Informed EMDR does not replace standard EMDR—it enriches it. It reminds us that trauma is not just what happened, but what was missing in the aftermath. And healing is not just about reprocessing memory, but about experiencing something new in relationship.
For many clients, especially those with complex trauma, this integration is the difference between symptom relief and true transformation.
Final Thoughts
Attachment-Focused Somatic-Informed EMDR offers a compassionate, relationally grounded pathway for trauma healing. It invites both clinician and client into a process that honors the nervous system, the story, and—most importantly—the need for connection.
In the words of Laurel Parnell, “When clients feel securely connected, their capacity to process trauma expands—and healing becomes not only possible, but sustainable.”
If this feels right for you, schedule a consultation or initial assessment!